COMPARISON OF PULSED FIELD ABLATION WITH A VARIABLE-LOOP CIRCULAR CATHETER AND VERY HIGH-POWER SHORT-DURATION RADIOFREQUENCY ABLATION FOR PULMONARY VEIN ISOLATION IN ATRIAL FIBRILLATION USING A NEAR-ZERO FLUOROSCOPY WORKFLOW: A RETROSPECTIVE SINGLE-CENTRE ANALYSIS
Background
Catheter ablation is an established therapy for atrial fibrillation (AF). Pulsed field ablation (PFA) and very high-power short-duration radiofrequency ablation with up to 90W (RFA) are established to achieve rapid and safe pulmonary vein isolation (PVI). Comparative data from a single center applying the same near-zero fluoroscopy workflow to both technologies are limited.
Objective
To retrospectively compare PFA via VLCC (VARIPULSE™) and high-power short-duration RFA (QDOT) for PVI with regard to procedural times, safety, and efficiency under a uniform near-zero fluoroscopy strategy.
Methods
We conducted a retrospective single-center analysis of the first 100 consecutive patients treated with PFA and the first 100 consecutive patients treated with QDOT-RFA to balance for learning-curves. Baseline characteristics were well balanced (p>0.05). The same near-zero fluoroscopy workflow based on 3D electroanatomical mapping was applied to both groups. Primary endpoints were acute complete PVI, total procedure time, and fluoroscopy parameters; secondary endpoints were periprocedural and in-hospital complications.
Results
Acute PVI was achieved in 100% of patients in both groups. Procedure times were short and clinically comparable (PFA 41 min vs RFA 44 min, p>0.05). Owing to the standardized near-zero fluoroscopy approach, fluoroscopy time and dose were low in both groups and did not differ significantly (p>0.05). No major procedure-related complications occurred; one clinically relevant access-site bleeding was observed in the RFA group.
Conclusion
In a single high-volume center using a uniform near-zero fluoroscopy workflow, both PFA and high-power short-duration RFA proved to be fast, safe, and efficient for PVI in AF. These findings support the use of either technology as a first-line (“first-do”) option when modern mapping-guided, low-radiation workflows are available. Long-term rhythm follow-up is warranted.
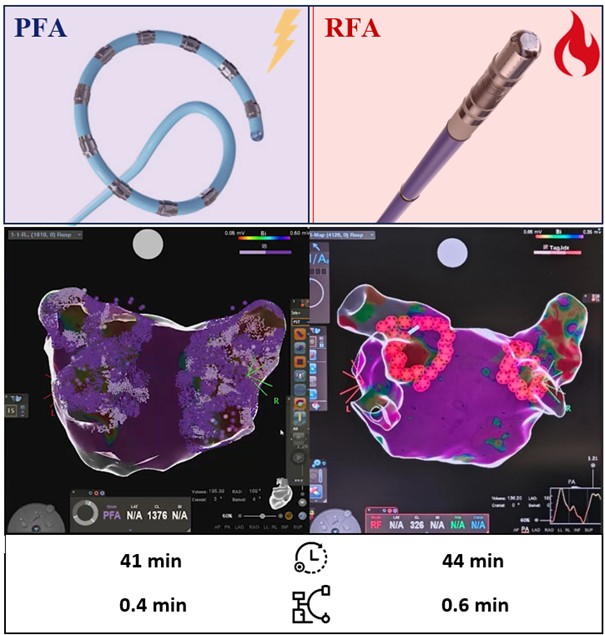
Central illustration



