Background
Transfemoral aortic valve replacement (TAVR) for severe aortic regurgitation (AR) in degenerated stentless aortic valve conduits remains technically challenging, particularly in the presence of anastomotic stenosis. According to the 2025 ESC/EACTS guidelines, transfemoral valve implantation may be considered (Class IIb, Level B) in patients with symptomatic severe AR who are deemed inoperable and present with suitable anatomy. In such cases, snare-assisted maneuvers can facilitate device advancement through tortuous or narrowed aortic segments.
Case Report
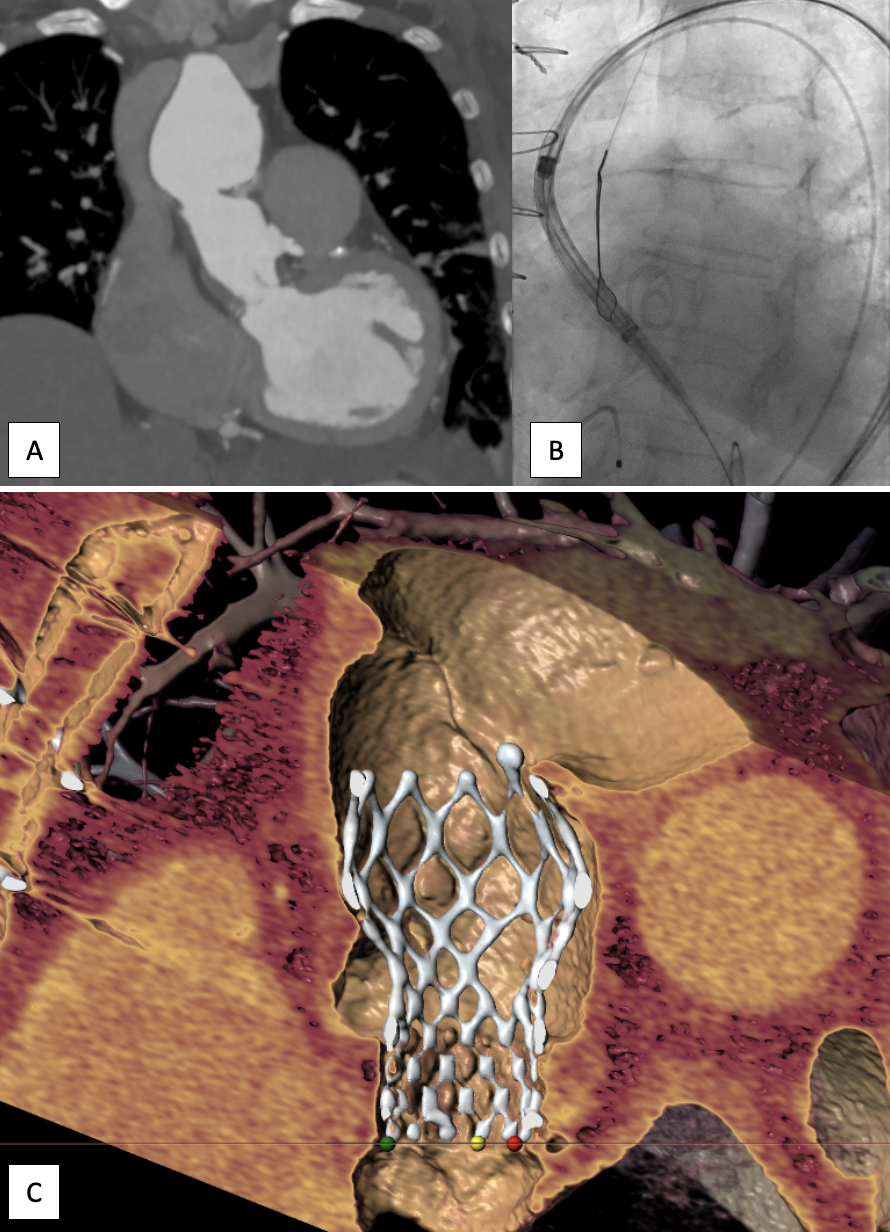
We report the case of an 84-year-old female presenting with rapidly progressive dyspnea (NYHA IV). Her medical history included prior Bentall surgery with stentless aortic valve Conduit (2006, Shelhigh bioprosthesis). Echocardiography revealed a flail right coronary cusp leaflet with severe eccentric AR and preserved biventricular function. Coronary angiography ruled out significant coronary artery disease. Computed tomography angiography demonstrated a pronounced angulation and anastomotic stenosis of the ascending aorta at the graft junction (fig. A). Given advanced age and elevated surgical risk, the heart team opted for transfemoral valve-in-valve TAVR supported by a snare maneuver to overcome the anastomotic stenosis.
The procedure was performed under general anesthesia and transesophageal echocardiography (TEE) guidance using bilateral femoral access. A 6F/30 mm Goose Neck snare was introduced via the left radial artery. Then balloon aortic valvuloplasty with an 18 mm SC-balloon was performed with simultaneous aortic root angiography to confirm appropriate prothesis sizing and demonstrate the location of the constrained portion of the valve at which anchoring would occur. Finally a 23 mm Evolut FX PLUS (Medtronic) prosthesis was advanced via the right femoral approach. In the aortic arch, the leading edge of the valve was captured with the snare catheter and gently guided across the stenotic anastomosis under controlled countertraction (fig. B). After successful crossing, the prosthesis was positioned at the annular level, released stepwise under TEE and fluoroscopic guidance, and post-dilated with an 18 mm SC-balloon (fig. C). Final angiography and echocardiography demonstrated an excellent procedural result (Gradient 13/7 mmHg) with only trace paravalvular AR.
Conclusion
This case illustrates that valve-in-valve TAVR represents a guideline-conform and safe therapeutic option in patients with degenerated aortic bioprosthesis and prohibitive surgical risk, even in the presence of challenging aortic anatomy. The snare-assisted maneuver enabled coaxial, controlled advancement of the prosthesis across a severe anastomotic stenosis, ensuring optimal positioning and outcome.