Background
Re-do pulmonary vein isolation (PVI) remains a challenge in patients with recurrent atrial fibrillation (AF). Conventional re-do ablation is performed using point-by-point radiofrequency (RF) energy applying touch-up lesions guided by a prior three-dimensional electroanatomic mapping. Novel ablation systems such as Affera™ and Faraview™ integrate high-resolution mapping and energy delivery within a single catheter so-called map&ablate (M&A). The aim of this study was to compare procedural performance in re-do PVI procedures using M&A systems vs. standard RF ablation (RFA).
Methods
This single-center retrospective study included 60 consecutive patients (n=20 per group) who underwent re-do PVI between January 2025 and November 2025 using 2 M&A systems (Affera™, Faraview™) and point-by-point RFA. Procedural characteristics, acute procedural success, and complication rates were analyzed.
Results
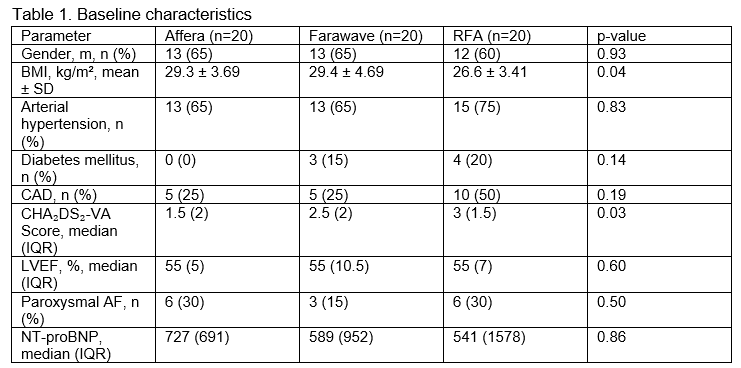
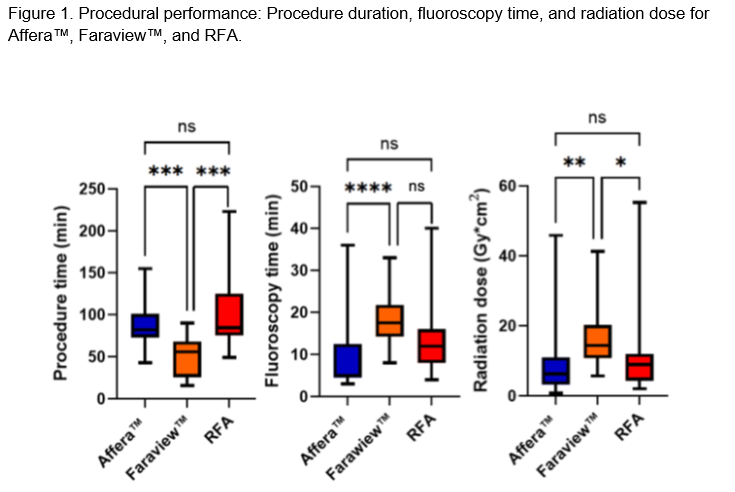
Baseline characteristics were comparable between groups except for a slightly lower BMI and higher CHA₂DS₂-VA score in the RFA cohort (Table 1). Procedure time was the shortest with Faraview™ (50.2 ± 23.7 min), followed by Affera™ (85.2 ± 25.6 min) and RFA (103 ± 43.6 min; p < 0.001) (Figure 1). In contrast, median fluoroscopy time and radiation exposure were lowest with Affera™ (5 [6] min; 6.34 [6.91] Gy·cm²) and highest with Farawave™ (17.5 [6.5] min; 14.4 [9.1] Gy·cm²; p ≤ 0.001) (Figure 1). Re-isolation of pulmonary vein gaps was required in 75% of Affera™ procedures, in all Faraview™ and RFA cases (p < 0.01). Additional ablation lesions were most frequently applied with Affera™ (85%) compared to Faraview™ (50%) and RFA (60%; p = 0.06), consisting of cavotricuspid isthmus, roof, anterior lines, and posterior wall isolation (PWI). PWI was performed in 55% of Affera™, 40% of Farawave™, and 15% of RFA patients (p=0.01). Acute procedural success was achieved in all Affera™ and Faraview ™ cases and in 95% of RFA cases. Of note, in one RFA procedure, tachyarrhythmia termination could not be achieved requiring electrical cardioversion due to excessive procedure duration. Periprocedural complications were rare, with a single vascular complication occurring in the RFA group. The use of >2 femoral sheaths was significantly higher with RFA (90%) compared to Affera™ (25%) and Faraview ™ (5%; p < 0.001).
Conclusion
In PVI repeat procedures, M&A system (Affera™ and Faraview™) demonstrated shorter procedure duration and required fewer femoral sheaths compared with conventional point-by-point RFA, while maintaining high acute efficacy and safety. Our data highlight the potential role of M&A systems in PVI re-do procedures in the future. However, larger cohorts and longer follow-up are warranted to evaluate long-term lesion durability and clinical outcome rates using these systems.