Patient presentation: An 83-year-old patient with dyslipidaemia, hypertension, smoking history, paroxysmal atrial fibrillation and prostate cancer presented with exertional angina to an external medical facility. Clinical examination, electrocardiography and laboratory analyses were unremarkable. Transthoracic echocardiography demonstrated preserved left-ventricular systolic function but inferior basal wall-motion abnormalities. Invasive coronary angiography revealed severe three-vessel coronary artery disease with heavily calcified stenoses involving the left main and left anterior descending arteries. During percutaneous coronary intervention on the proximal and distal left anterior descending artery, an iatrogenic left main dissection occurred, prompting immediate transfer to our tertiary care center for further urgent management.
Initial work up: Upon arrival, the patient remained haemodynamically stable but required emergency coronary intervention. Angiography confirmed a dissection extending from the distal left main into the proximal left anterior descending arteries. Intravascular ultrasound was utilised to define lesion morphology and optimise procedural strategy. Sequential non-compliant balloon dilatations were followed by high-pressure post-dilatations to ensure vessel expansion. Extensive calcification required intravascular lithotripsy.
Diagnosis and management: To restore coronary integrity and prevent contrast dye extravasation, multiple covered coronary stents were implanted fromthe left main into the left anterior descending artery with complete sealing of the dissection fl ap. However, shortly thereafter,the patient developed hypotension with echocardiographic evidence of a rapidly accumulating pericardial effusion consistentwith tamponade physiology. Emergency pericardiocentesis via a subxiphoid puncture was performed and resulted inimmediate haemodynamic stabilisation. Angiography concluded with restored TIMI 3 coronary fl ow and preserved myocardialperfusion.
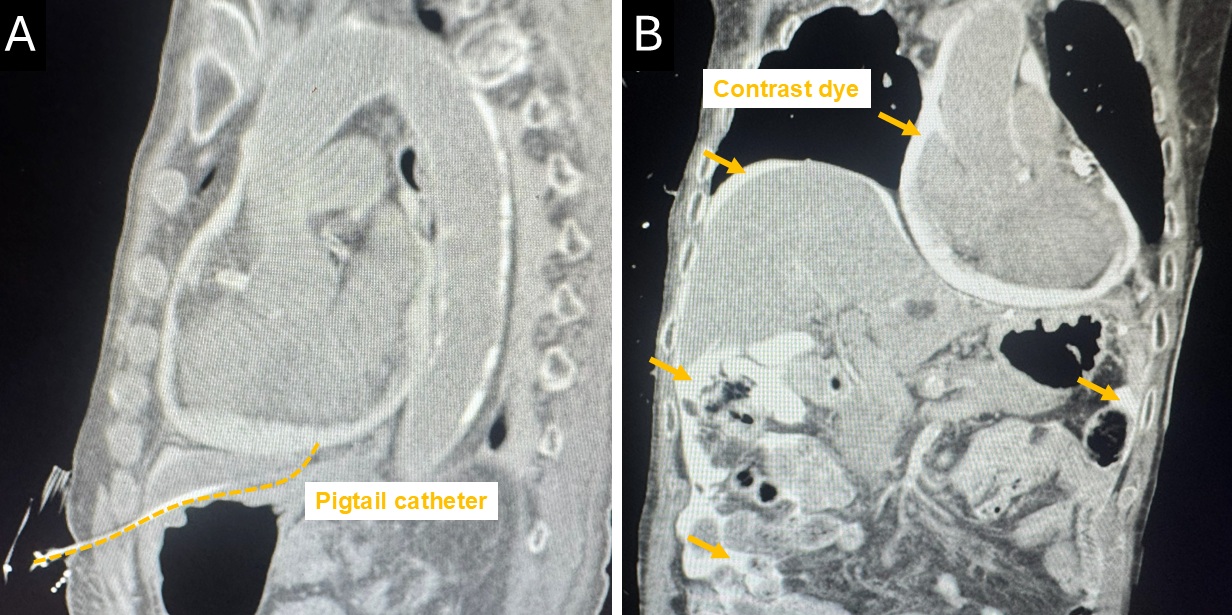
Follow-up: Post-procedural computed tomography, performed due to persistent abdominal discomfort, revealed contrast dye leakage intothe peritoneal cavity across multiple quadrants. The imaging confi rmed that the pericardial drainage catheter had perforatedthe peritoneum, resulting in an iatrogenic pericardio-peritoneal fi stula. Serial echocardiography showed only a minimal, stableresidual pericardial effusion without recurrent signs of tamponade. Consequently, the drainage catheter was removed earlyand repeat computed tomography demonstrated progressive resolution of intraperitoneal contrast dye. The patient recovereduneventfully and was discharged without further complications at follow-up.
Conclusions: This case illustrates the complexity of high-risk percutaneous coronary intervention and underscores the necessity for vigilantperi-procedural monitoring to identify unexpected causes of haemodynamic compromise. Peritoneal perforation duringsubxiphoid pericardiocentesis represents a rare but clinically signifi cant complication that can result in ineffective pericardialdrainage. When clinical presentation and echocardiographic fi ndings are discordant, cross-sectional imaging becomesessential to confi rm catheter position and detect abnormal fl uid communication. Early recognition of a pericardio-peritonealfi stula and prompt removal of the misplaced catheter can prevent further deterioration and potentially obviate the need forsurgical intervention. Multidisciplinary, guideline-directed decision-making remains crucial to ensure safe and effectivemanagement in complex pericardial emergencies.