AIMS: Right ventricular (RV) systolic function is an independent determinant of outcomes in various diseases, yet its assessment remains challenging especially under altered loading conditions. Invasive pressure-volume loop (PVL) analysis provides the reference standard for evaluating load-independent RV contractility. Although heart failure with preserved ejection fraction (HFpEF) is primarily considered a left ventricular entity, growing evidence indicates biventricular involvement. We therefore aimed to characterize load-independent RV systolic function using invasive PVL analysis, develop a non-invasive PVL approach, and assess its prognostic relevance in HFpEF.
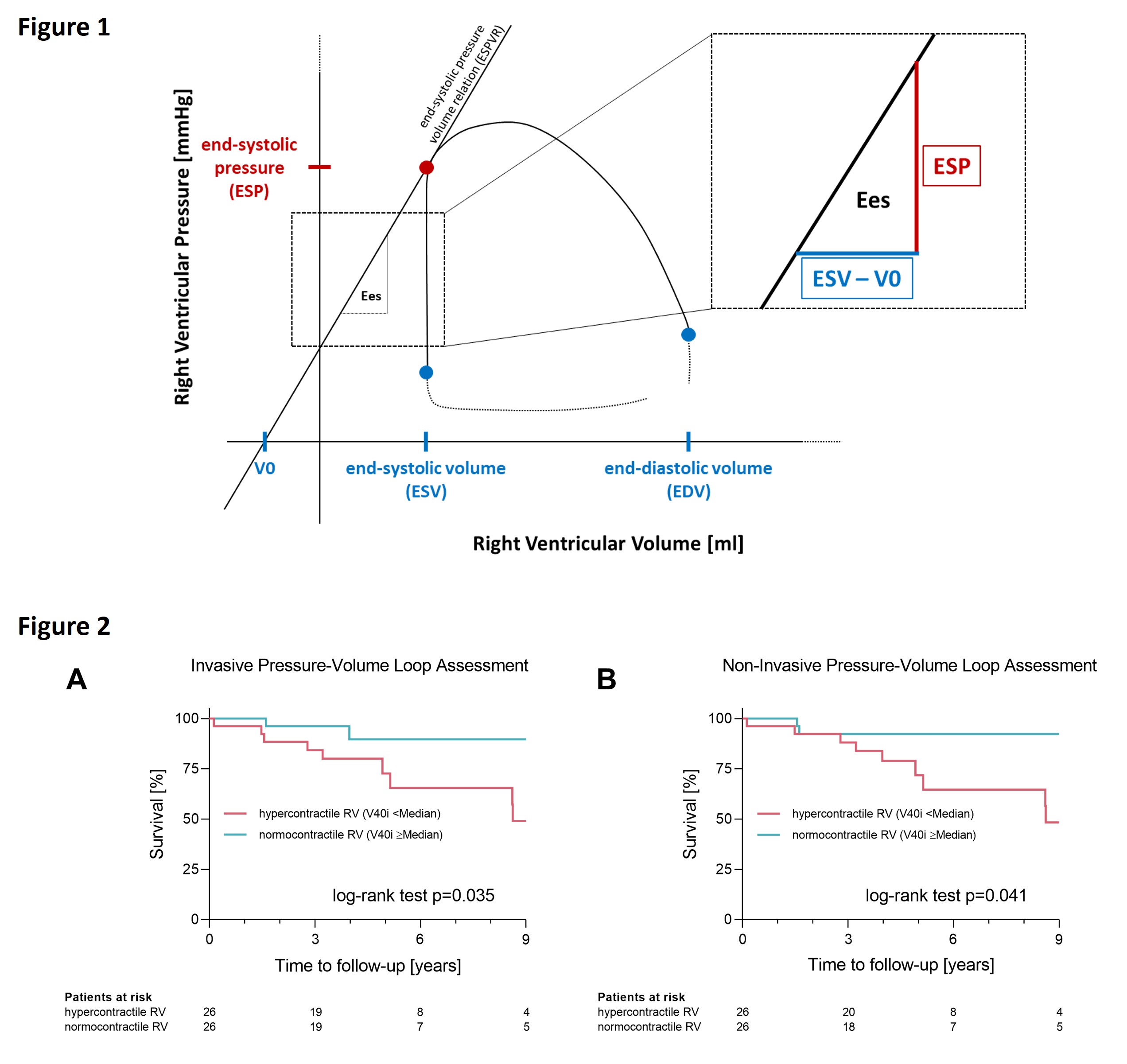
METHODS: Patients with HFpEF underwent transthoracic echocardiography and cardiac magnetic resonance imaging (CMR) before invasive assessment. During right heart catheterization, RV-PVL analysis was performed at rest and during preload reduction to determine end-systolic elastance (Ees) and the volume-axis intercept (V0) of the end-systolic pressure-volume relationship (ESPVR, Fig. 1A). From both, we calculated the indexed RV volume at an end-systolic pressure of 40 mmHg (RV-V40i) as a quantitative, load-independent index of RV systolic function, with lower values indicating higher contractility. Non-invasive PVLs were derived using correlations from invasive data combined with imaging parameters. Survival analyses were performed according to median invasive and non-invasive RV-V40i.
RESULTS: Fifty-two patients (median age 72 years [IQR 68 to 77], 67% female) were included (median follow-up 1,654 days [IQR 1,150 to 3,249]). PVL-derived RV-ESP was 18% lower than RV systolic pressure and was estimated non-invasively using echocardiographic systolic pulmonary artery pressure. RV end-systolic volume correlated strongly with RV-V0 (r=0.75, p<0.001) and was used for its non-invasive estimation.
Invasive and non-invasive PVL parameters demonstrated strong correlations for RV-ESP (r=0.95, p<0.001), RV-V0 (r=0.75, p<0.001), RV-Ees (r=0.73, p<0.001) and RV-V40i (r=0.85, p<0.001).
Hypercontractile RV HFpEF (RV-V40i <median) patients were more frequently female (85% vs. 50%, p=0.008) compared to those with normocontractile RV HFpEF (RV-V40i ≥median), whereas other baseline characteristics did not differ significantly. In hypercontractile patients on CMR, RV volumes were smaller (EDV index 63ml/m² [IQR 58 to 77] vs. 70ml/m² [IQR 63 to 85], p=0.041) and RV-EF was higher (64% [IQR 55 to 68] vs. 57% [IQR 47 to 61], p=0.010). Kaplan-Meier analysis revealed worse survival in patients with hypercontractile RVs, irrespective of invasive (p=0.035) or non-invasive (p=0.041) PVL analysis (Fig. 2A+B).
CONCLUSION: Beyond diastolic stiffness, hypercontractility is increasingly recognized as a key feature of HFpEF pathophysiology. RV hypercontractility appears to be more than a compensatory response. It is an independent determinant of long-term survival in HFpEF. Contrary to the conventional assumption that better RV systolic function predicts improved outcomes, patients with RV hypercontractility showed higher mortality, likely reflecting increased RV afterload. The proposed concept of non-invasive RV PVL assessment bares the potential for broader application across cardiovascular diseases fostering our understanding of HFpEF.