Background: In patients with heart failure with preserved ejection fraction (HFpEF), most pharmacological therapies (spironolactone, candesartan, sacubitril/valsartan) have only been shown to be effective in patients with left ventricular ejection fraction (LVEF) lower than approximately 55%. In contrast, pharmacological agents that primarily target peripheral limitations have also been shown to be effective among patients with higher LVEF (e.g., empagliflozin, dapagliflozin and semaglutide). One of the most effective treatments to target exercise intolerance, the cardinal symptom of HFpEF, is regular exercise training. However, it is not known whether exercise training benefits depend on baseline LVEF.
Purpose: To evaluate the effects of exercise training on peak oxygen consumption (V̇O2) according to resting baseline LVEF in patients with HFpEF.
Methods: For this analysis, combined data sets from two of the largest exercise training trials performed in HFpEF to date. In the OptimEx-Clin trial, 180 patients were randomized (1:1:1) to 12 months of high-intensity interval training (3× per week for 38 min), moderate continuous training (5× per week for 40 min) or usual care. In the Ex-DHF trial, 322 patients were randomized (1:1) to 12 months of endurance training (3× per week with increasing session duration from 30-60 min) and resistance training (2× per week, starting at week 5) versus usual care. For the present analysis, all exercise training groups and both control groups were combined into one exercise and one control group. Peak V̇O2 was defined as the highest 10-second average during symptom-limited incremental cardiopulmonary exercise testing. The association between change in peak V̇O2 after 12 months and baseline resting LVEF was analyzed using linear regression analysis with main effects of baseline LVEF and group as well as their interaction term. Moreover, patients were grouped into LVEF categories (50-54%, 55-59%, 60-64% and ≥65%) and compared using independent t-tests. All analyses were performed using R Statistical Software with significance levels of α = 0.05.
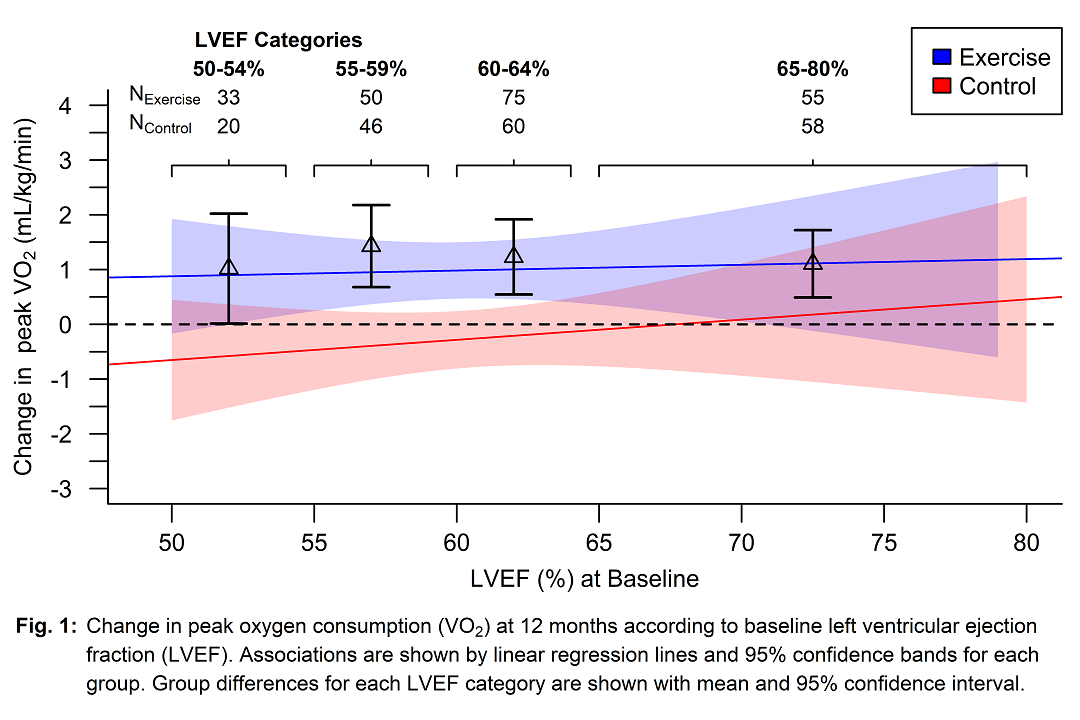
Results: Among 502 randomized patients, 397 had paired peak V̇O2 measurements both at baseline and at 12-month follow-up (60.5% women; mean age, 70 years; mean LVEF, 60%) and were included in this secondary analysis. At 12 months, the change in peak V̇O2 was significantly different between exercise training and usual care [mean difference, 1.2 mL/kg/min (95% CI, 0.5 to 1.9), P=0.001], with no significant main effect for LVEF (P=0.58). The change in peak V̇O2 was similar across the LVEF.F continuum (interaction P=0.72) with significant improvements with exercise training for all LVEF categories (Fig. 1).
Conclusion: In patients with HFpEF, 12 months of exercise training significantly improved peak V̇O2 compared with usual care to a similar extent across the LVEF continuum (50-80%). These data support the application of exercise training in patients with HFpEF regardless of LVEF.