Background. In mitral transcatheter edge-to-edge repair (TEER), operators face the dilemma of optimizing TEER results by additional devices at expenses of increasing post-procedural mean mitral valve pressure gradient (MPG). The impact of post-procedural hemodynamic results following mitral TEER in primary MR is still matter of debate. While the severity of residual MR (rMR) after TEER is a well-known predictor of adverse outcomes, data on the prognostic impact of MPG are still conflicting. Finding an ideal balance between these two parameters could substantially improve procedural guidance and decision-making.
Aims. We sought to evaluate the association between post-procedural rMR and MPG, measured by transesophageal echocardiography at the end of the procedure, as well as their individual and combined impact on clinical outcomes among patients who underwent TEER for severe primary MR.
Methods
The PRIME-MR registry includes 2,873 patients with severe primary MR undergoing mitral TEER from 2008-2022 at 25 international sites. Clinical outcomes were assessed according to post-procedural rMR severity and MPG. Patients with available data on both parameters were categorized according to rMR (optimal result [OR]: ≤1+, suboptimal result [SR]: ≥2+) and MPG (low gradient [LG]: ≤5mmHg, high gradient [HG]: >5mmHg). The prognostic impact of rMR and MPG was evaluated in a Cox regression analysis adjusting for conventional risk (age, sex, atrial fibrillation, left ventricular ejection fraction, chronic kidney disease, chronic obstructive pulmonary disease), and rMR or MPG, respectively. The primary endpoint was the composite of all-cause mortality and heart failure hospitalization at 2 years. Median follow-up was 2.02 (95%-CI 1.92-2.11) years.
Results
Post-procedural rMR and MPG were available in 2,068 and 1,460 patients undergoing TEER for primary MR, respectively. Kaplan-Meier analysis according to rMR severity showed significant differences for the primary endpoint at 2 years between patients with rMR ≤1+ (28.5%), 2+ (40.5%) and ≥3+ (56.2%, p<0.001). Similarly, the primary endpoint occurred less frequent in patients with post-procedural MPG ≤5 mmHg (31.4%) compared to patients with MPG >5 mmHg (41.6%, p=0.075), without reaching statistical significance.
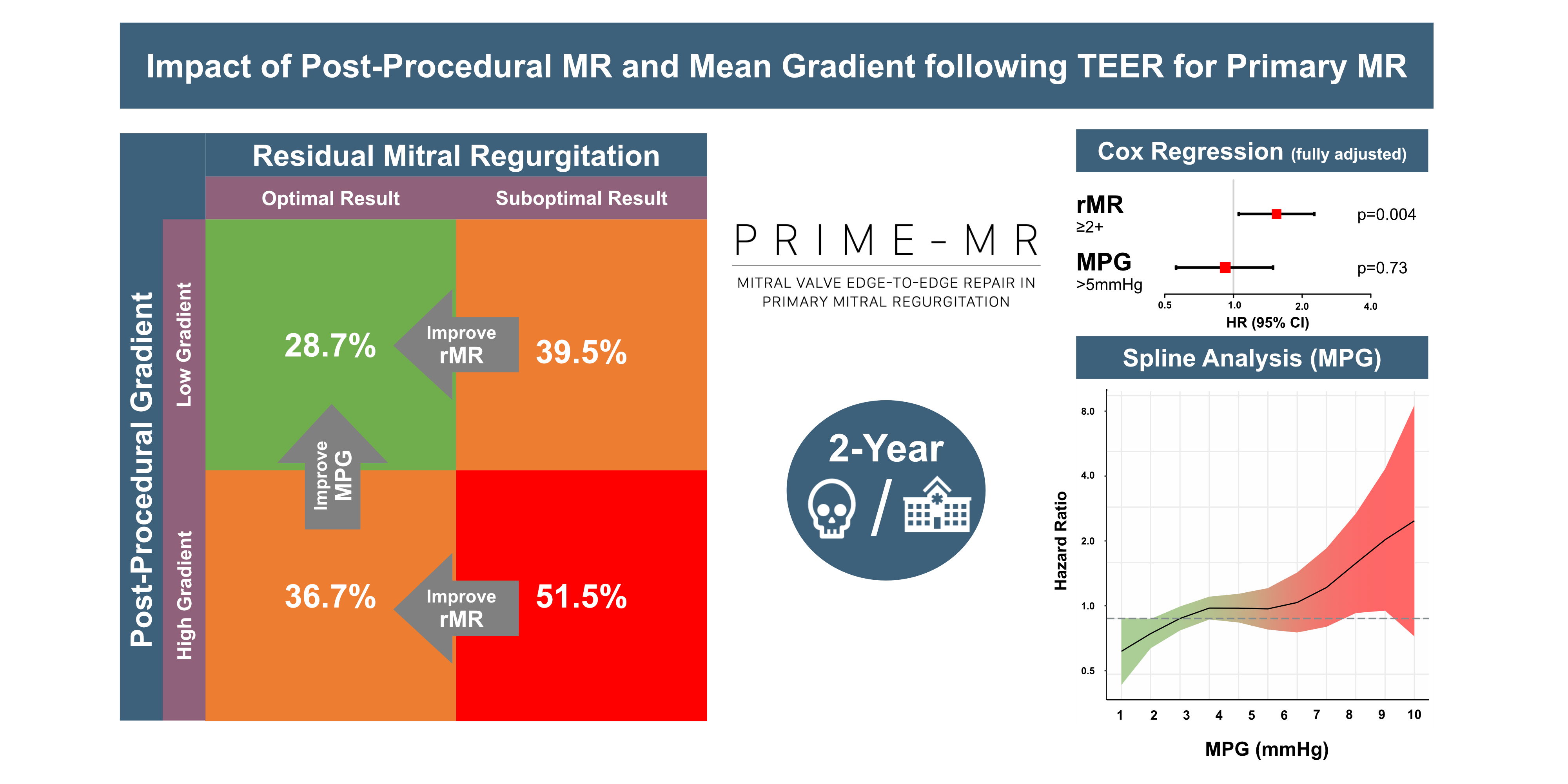
Both, post-procedural rMR and MPG were available in 1,453 patients. Four subgroups according to rMR and MPG were compared: OR/LG (n=1,009), OR/HG (n=96), SR/LG (n=299), and SR/HG (n=49). The primary endpoint occurred in 28.7% (OR/LG), 36.7% (OR/HG), 39.5% (SR/LG) and 51.5% (SR/HG, p<0.001). Following Cox regression, rMR ≥2+ was independently associated with the primary endpoint at 2 years (HR 1.62, 95%-CI 1.16-2.26, p=0.004), whereas MPG >5 mmHg did not show a significant association (HR 0.92, 95%-CI 0.56-1.49, p=0.73).
Conclusions
Based on data from a large real-world registry, only post-procedural rMR, but not MPG, independently predicted long-term clinical outcomes following TEER for primary MR. When performing TEER in primary MR, both rMR and MPG should be assessed and accounted for. However, in a real-world scenario where only one appears achievable, an optimal rMR result seems to outweigh the impact of mean transvalvular gradients.