Background:
Transcatheter aortic valve implantation (TAVI) is an effective treatment option for symptomatic aortic valve stenosis (AS). The JenaValve Trilogy system (JVTS; JenaValve Technology, Irvine, CA) is a CE-marked, short-frame, self-expanding TAVI device designed for transfemoral procedures in patients with AS or aortic regurgitation. Recent studies demonstrate excellent hemodynamics and minimal paravalvular regurgitation in patients with symptomatic aortic regurgitation treated with the JVTS. The ACURATE neo2 (Neo2; Boston Scientific, Marlborough, MA, USA) is a next-generation, self-expanding TAVI device featuring external porcine pericardial sealing skirts designed to reduce paravalvular regurgitation. Recent registry studies have demonstrated promising valve hemodynamics associated with this device. Thus, this study aimed to compare the procedural characteristics and hemodynamic outcomes in patients with AS undergoing TAVI using the JVTS and the Neo2 devices.
Methods:
Forty-two patients with AS underwent transfemoral TAVI with the JVTS at six German centers, while eighty patients received transfemoral TAVI for AS using the Neo2 device at the University Hospital Cologne. Optimal full matching resulted in 35 patients in the JVTS group and all 80 patients in the Neo2 group in this preliminary study. Site-reported discharge echocardiograms were used to assess echocardiographic outcomes.
Results:
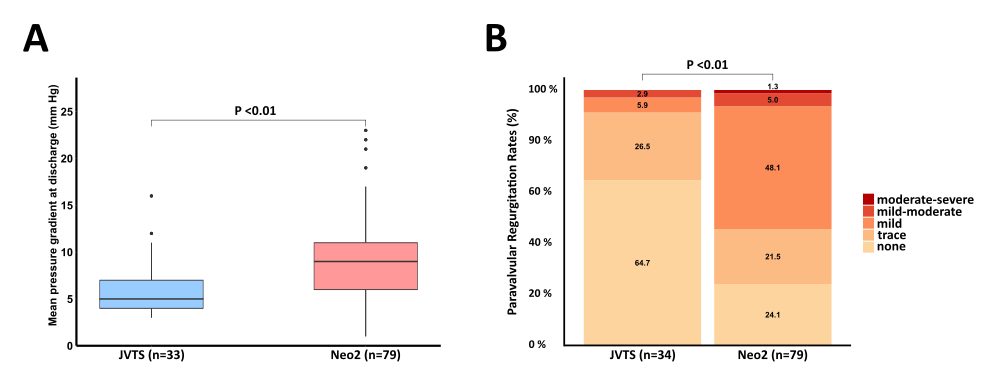
The median age was 82.7 ± 5 years, with 70% of the patients being female. The mean aortic perimeter was 73.2 ± 5.1 mm, and the aortic valve area was 0.72 ± 0.19 (n = 2 missing). Patients undergoing TAVI with the JVTS less frequently underwent predilatation (JVTS: 77% vs. Neo2: 99%; P < 0.001). The rates of postdilation were similar (JVTS: 20% vs. Neo2: 18%; P < 0.75). Procedural duration (JVTS: 75.8 ± 29.5 min vs. Neo2: 53.2 ± 20.9 min; P < 0.001), radiation time (JVTS: 19.9 ± 7.2 min vs. Neo2: 14.9 ± 6.5 min; P < 0.001), and contrast usage (JVTS: 144.7 ± 51.7 ml vs. Neo2: 109.0 ± 34.6 ml; P < 0.001) were higher in patients treated with the JVTS. The rates of new permanent pacemaker implantation (JVTS: 2.9% vs. Neo2: 7.5%; P = 0.67) showed numerical differences without reaching statistical significance in this small cohort. The mean pressure gradient at discharge (Figure 1a) and the rates of paravalvular regurgitation (Figure 1b) were significantly lower with the JVTS.
Conclusion:
In this small, preliminary study involving patients with AS, TAVI using the JVTS resulted in longer procedural durations, increased radiation time, and higher contrast usage compared to the Neo2. However, patients treated with the JVTS exhibited significantly lower rates of paravalvular regurgitation and reduced mean pressure gradients compared to those receiving the Neo2 device.