Background: Primary percutaneous coronary intervention (PPCI) is the preferred reperfusion strategy in patients with ST-segment elevation myocardial infarction (STEMI) and symptom on-set within 48h. Patients ≥80 years old were excluded or underrepresented in trials supporting PPCI. In recent international real-world STEMI registries dominated by data from the United States only 30% of these elderly were triaged to PPCI – indicating a potential underuse. To date, it is uncertain whether PPCI is equally effective in this more morbid and frailer patient group or might even cause harm.
Objective: This study examined the historical and contemporary treatment trends of the elderly with STEMI. Efficacy and safety data were analyzed to assess whether PPCI is indicated in this vulnerable patient group.
Methods: The multicentric, metropolitan registry included STEMI patients treated between January 2005 and December 2020. Patients ≥80 years were defined as “the elderly”, younger patients (<80 years) formed the comparator group. Data were analyzed using Student’s t, Mann Whitney U, and Chi square test. A two-sided p-value < 0.05 was defined as statistically significant.
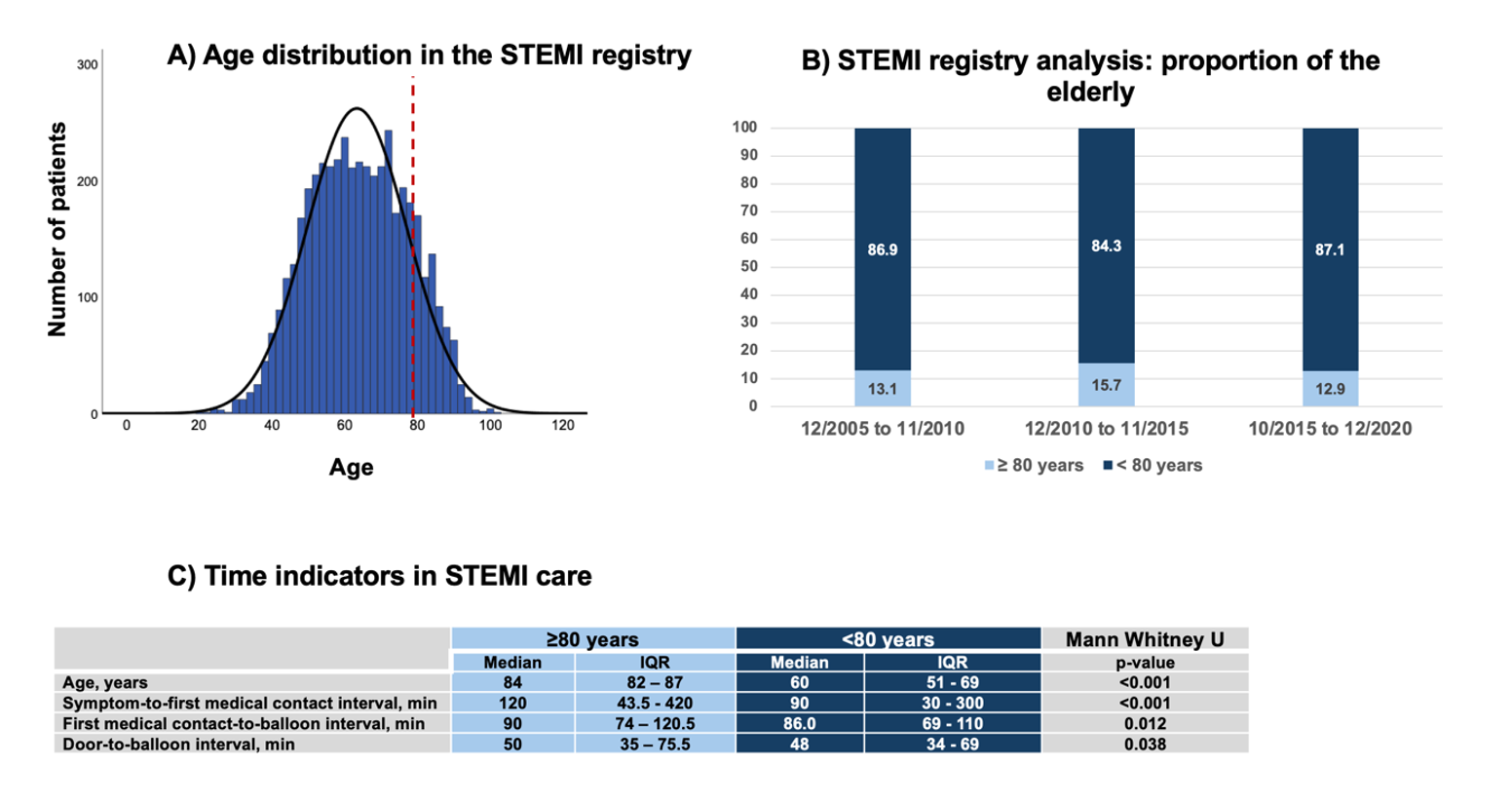
Results: In total, 4768 patients were included in the STEMI registry. Of these, 624 (13.1%) were ≥80 years old and were classified as “the elderly” (see A). The proportion of the elderly was consistent over the considered period (see B).
The median age was 84.0 years (IQR 82.0 – 87.0) with a maximum of 101 years in the elderly. Specifically, 88.6% were octogenarians, 10.9% were nonagenarians and 0.5% were centenarians. Every second patient in the elderly was female, while women represented only 25.8% in the total STEMI registry cohort.
The median symptom-to-first medical contact interval was remarkably longer in the elderly compared to younger patients (120 vs. 90 minutes, p<0.001). All other time indicators were numerically comparable between the groups, but still statistically significantly different, and favoring younger patients (see C).
The elderly were usually referred for immediate coronary angiography (96.8%), but a culprit lesion was less frequently detected compared to younger patients (85.8 vs. 89.3%, p<0.02). Correspondingly, stent implantation was less often performed in the elderly (74.0 vs. 83.2%, p<0.001).
Every fifth elderly patient died during index hospitalization. In-hospital mortality was the highest among centenarians (33.3%) and nonagenarians (26.5%). Octogenarians had an in-hospital mortality rate of 20.7%. Consequently, in-hospital mortality was higher as in younger patients (21.3 vs. 7.7% p<0.001).
Access site hemorrhage was the safety outcome. It was a rare event affecting 1.5% of the elderly and 0.9% of younger patients (p=0.144).
Conclusion: In contrast to contemporary international registry data, triage of the elderly to PPCI was the standard of care in this metropolitan STEMI registry.
PPCI was associated with low access site hemorrhage and acceptable short-term survival rates. Consequently, PPCI should not automatically be withheld.
A more selective triage beyond age boundaries should be prospectively evaluated. Future trials should also systematically evaluate whether PPCI is also associated with a more favorable long-term prognosis and a gain of quality of life. In the meantime, it will be crucial to encourage the elderly to immediately seek medical advice in the presence of ischemic symptoms to overcome the more distinct patient related delay.