Background: Transcatheter Edge-to-Edge Repair (TEER) is an established therapy for patients with symptomatic high-grade mitral regurgitation (MR) and has been validated for the treatment of both functional and degenerative MR. However, there are relevant differences in clinical characteristics between the two etiologies and date on their impact on long-term survival are scarce. Therefore, we aimed to investigate the influence of MR etiology on survival after TEER.
Methods: In this multicenter cohort study, 725 patients from four German heart centers were investigated between 2011-2022. Patients were stratified according to MR etiology. Degenerative MR was present in the case of any structural alteration of the valvular apparatus. Functional MR was further divided into ventricular functional (v-FMR) and atrial functional MR (a-FMR). The former existed in the case of impaired LV function and/or LV dilatation, the latter was present in the case of LA dilatation with preserved LV function and structure. Survival time analysis was performed by using the Kaplan-Meier method.
Results: The majority of 59.6% of patients (432/725) had functional MR, which were further separated into v-FMR in 50.6% (367/725) and a-FMR in 9% (65/725) of patients. Patients with v-FMR were significantly younger, were more frequently male and had a significantly higher prevalence of CAD. Corresponding to the definition of FMR subtypes, lower LV function with higher numbers of implanted devices was seen among patients with v-FMR, as presented in
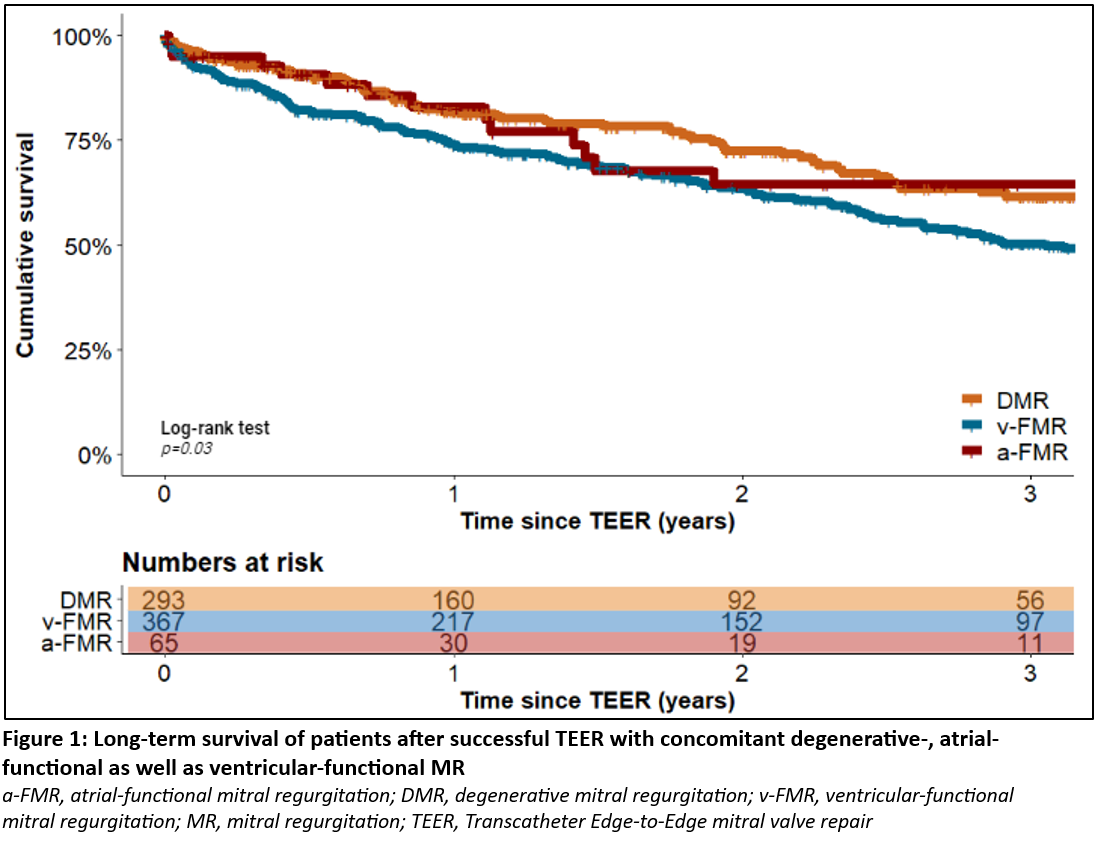
Table 1. Patients with v-FMR had the poorest long-term survival while those between patients having a-FMR and degenerative MR did not differ significantly, as illustrated in
Figure 1 and Table 2.
Conclusion: Our data from a “real-world” collective emphasize that patients with v-FMR exhibit important differences in comorbidities and long-term survival compared to the further MR etiologies.
Table 1: Clinical data of patients undergoing TEER with concomitant degenerative-, atrial-functional and ventricular-functional mitral regurgitation
|
Variable
|
Overall
(n=725)
|
DMR
(n=293)
|
v-FMR
(n=367)
|
a-FMR
(n=65)
|
p-value
|
|
Age (years)
|
78 ± 8
|
80 ± 7
|
77 ± 8
|
81 ± 7
|
<0.0001
|
|
Male sex
|
63.3% (459)
|
59.4% (174)
|
69.2% (254)
|
48.4% (31)
|
0.001
|
|
euroSCORE (%)*
|
16% (21)
|
13.8% (17.5)
|
20.1% (25)
|
7.9% (10)
|
<0.0001
|
|
CAD
|
62.6% (454)
|
56% (164)
|
68.4% (251)
|
60.9% (39)
|
0.004
|
|
Pre-existing ICD
|
23.2% (168)
|
14.3% (42)
|
34.1% (125)
|
1.6% (1)
|
<0.0001
|
|
Pre-existing CRT
|
14.8% (107)
|
10.6% (31)
|
20.2% (74)
|
3.1% (2)
|
<0.0001
|
|
GFR (mL/Min)
|
50 ± 26
|
52 ± 30
|
47 ± 21
|
55 ± 24
|
0.1
|
|
NT-proBNP (ng/L)*
|
2788 (5234)
|
2467 (4786)
|
3493 (6068)
|
1434 (2150)
|
<0.0001
|
|
LVEF (%)
|
41 ± 15
|
46 ± 14
|
34 ± 12
|
59 ± 4
|
<0.0001
|
*Median + IQR
Table 2: Independent predictors of mortality in multivariable Cox regression analysis
|
Variable
|
Hazard Ratio
|
95%-CI
|
p-value
|
|
TR grade III
|
1.8
|
1.3-2.3
|
<0.001
|
|
NYHA class IV
|
1.5
|
1.2-2.0
|
0.003
|
|
Male sex
|
1.5
|
1.2-2.0
|
0.002
|
|
COPD
|
1.5
|
1.2-2.0
|
0.002
|
|
GFR <30mL/min
|
1.3
|
1.1-1.9
|
0.01
|
| v-FMR
|
1.4
|
1.1-1.8
|
0.007
|