Background and purpose
Abnormalities in mitral valve (MV) morphology are common in hypertrophic obstructive cardiomyopathy (HOCM) and are associated with the presence of MV systolic anterior motion (SAM) and left ventricular outflow tract (LVOT) obstruction. Percutaneous transluminal septal myocardial ablation (PTSMA) can efficiently reduce LVOT gradient. However, the impact of PTSMA on mitral valve annulus and leaflets has been rarely investigated. Our study aimed to assess the remodeling of mitral valve geometry after PTSMA in HOCM patients.
Methods
This retrospective study included HOCM patients who underwent PTSMA between 2021 and 2024 in the cardiology department of the University Hospital Würzburg. The MV structure was recorded by real-time 3D transthoracic echocardiography and a semi-automated quantitative analysis of MV annulus and leaflets was performed using EchoPAC (4D Auto MVQ, GE Healthcare).
Results
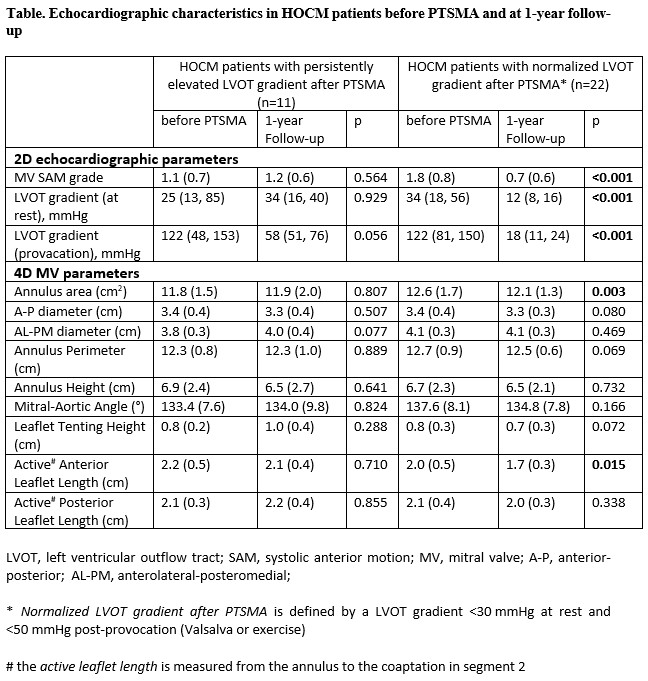
A total of 33 symptomatic HOCM patients (58(15) years, 61% men, LVEF 67(7)%) were included in our analysis. After 1-year follow-up, 22 patients (67%) demonstrated a significant reduction in LVOT gradient under both resting (34 (18, 56) mmHg vs. 12 (8, 16) mmHg, P<0.001) and provoked conditions (122 (81, 150) mmHg vs. 18 (11, 24) mmHg, P<0.001) (table). Further, in these patients, a decrease in SAM grade (1.8 (0.8) vs. 0.7 (0.6), P<0.001) and a reverse remodeling of MV were observed after PTSMA, reflected in a reduction in both annular and leaflet dimensions: annulus area decreased from 12.6 (1.7) cm2 to 12.1 (1.3) cm2 (P=0.003) and active anterior leaflet length decreased from 2.0 (0.5) cm to 1.7 (0.3) cm (P=0.015). In contrast, 11 patients showed persistent LVOT gradients either at rest or after provocation. In these patients, no significant difference in SAM grade as well as in mitral annulus and leaflet parameters was observed between baseline and follow-up (table).
Conclusions
In a well characterized sample of HOCM patients undergoing PTSMA we observed a significant conformational change of the MV after one year in patients who achieved a sustained LVOT gradient reduction. The decrease in active anterior leaflet length, together with reductions in LVOT gradient and SAM severity, highlight the complex dynamic interplay between mitral valve, interventricular septum and LVOT gradient in HOCM.