Aims: Maximally provoked LVOT obstruction (LVOTO) guides the management for patients with obstructive hypertrophic cardiomyopathy (HCM). Current guidelines recommend several provocation maneuvers, with exercise stress echocardiography (ESE) considered the preferred approach when other methods fail to induce LVOTO. This study compared commonly used maneuvers and explored handgrip exercise as a potential alternative to induce LVOTO.
Methods and results: In this prospective study, 20 patients with obstructive HCM underwent transthoracic echocardiography (TTE) with continuous wave Doppler assessment of LVOT gradients at rest and during the Valsalva maneuver, isometric handgrip exercise at 30% and 50% of maximal strength, squatting exercise, and bicycle ESE. The mean LVOT gradient at rest was 38.9 ± 31.4 mmHg. Handgrip exercise did not significantly alter gradients. In contrast, Valsalva (98.9 ± 52.8 mmHg), squatting (120.3 ± 68.8 mmHg), and bicycle ESE (83.4 ± 43.3 mmHg) all produced significant increases (p < 0.001 vs. rest) without a significant difference among these three maneuvers (Figure 1). Squatting elicited the highest gradient in 50% of patients. Procedure time was shortest with Valsalva (15 s) and squatting (1 min 23 s ± 28 s), compared with bicycle ESE (15 min 54 s ± 5 min 46 s; p < 0.001) (Figure 2).
Conclusion: The Valsalva maneuver, squatting, and bicycle ESE are similarly effective in provoking LVOTO, whereas isometric handgrip does not reliably induce LVOTO. Given its ease of use, low cost, and brief testing time, squatting may represent a practical alternative to bicycle ESE for routine clinical evaluation of LVOTO in obstructive HCM.
Figure 1
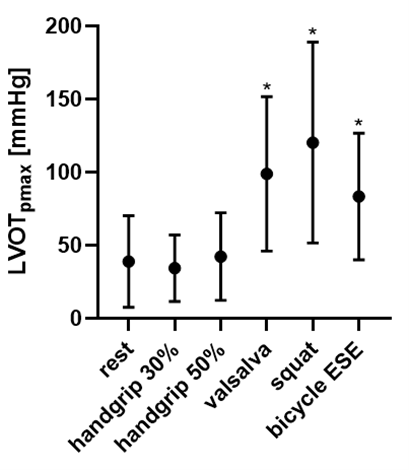
Figure 1. Peak LVOT gradients at rest and during different exercise modalities. Data points show mean values ± standard deviation. An asterisk (*) indicates statistical significance (p < 0.05) compared with resting peak LVOT gradient. ESE: exercise stress echocardiography.
Figure 2

Figure 2. Duration of three guideline-recommended provocation maneuvers, presented in minutes as mean ± standard deviation. An asterisk (*) denotes a statistically significant difference (p < 0.05) for this maneuver compared with each of the other exercise modalities individually. ESE: exercise stress echocardiography.



