1University Hospital Gasthuisberg Dept. of Cardiology Leuven, Belgien; 2University of Medicine and Pharmacy Department of Cardiology Craiova, Rumänien; 3Cardiovascular Research Institute Maastricht Department of Biomedical Engineering Maastricht, Deutschland; 4CHU Rennes Dept. of Cardiology Rennes, Frankreich
Introduction
The current eligibility criteria for cardiac resynchronization therapy (CRT) are a reduced left ventricular ejection fraction (LVEF ≤35%) and a bundle branch block (QRS ≥130ms). The QRS duration and morphology further determine the level of recommendation for CRT. Data shows that patients with septal flash or apical rocking, or both (SFoAR) on echocardiography have improved outcome after CRT regardless of QRS duration and morphology.
Purpose
To confirm that the visual assessment of septal flash and apical rocking provides incremental information to current guideline criteria.
To determine if the presence of SFoAR may warrant the highest level of recommendation for CRT regardless of QRS duration and morphology.
Methods
We analysed data in a multicentre, retrospective study from 220 patients referred for CRT according to guidelines.
Septal flash and apical rocking were assessed visually on echocardiography in the apical chamber views. Septal flash was defined as a short-lived inward motion of the interventricular septum into the left ventricle during the pre-ejection phase. Apical rocking was defined as a septal-to-lateral motion of the apex during ejection.
All patients were categorized according to SFoAR (yes/no).
All patients were categorized according to SFoAR (yes/no).
The hazard ratio (HR) for all-cause mortality or heart transplant after CRT implantation was determined using Cox proportional hazards regression analysis.
Models were adjusted for QRS duration and QRS morphology in addition to age, gender, atrial fibrillation/flutter, ischemic heart disease, and use of a defibrillator.
Sensitivity analyses were performed in patients with QRS duration of 130-149ms (n=59) and in patients with a non-LBBB morphology (n=40).
Results
At baseline 70% of patients presented with SFoAR. Median follow-up time after CRT was 5.1 [3.6 - 6.6] years. All-time, all-cause mortality was 34% (n = 62) and 1% (n = 3) had a heart transplant. In the full cohort, patients with SFoAR had a reduced risk for all-cause mortality or heart transplant (HR = 0.34; p < 0.001).
Sensitivity analysis revealed these results were consistent in patients with a QRS duration of 130-149ms (SFoAR HR = 0.19; p = 0.024) and in patients with a non-LBBB morphology (SFoAR HR = 0.16; p = 0.026). See Figure 1.
Sensitivity analysis revealed these results were consistent in patients with a QRS duration of 130-149ms (SFoAR HR = 0.19; p = 0.024) and in patients with a non-LBBB morphology (SFoAR HR = 0.16; p = 0.026). See Figure 1.
Conclusion
Patients with a guideline indication for CRT and the visual presence of septal flash or apical rocking (SFoAR) on echocardiography had a favourable long-term outcome regardless of QRS duration and morphology. Our results suggests patients with SFoAR should receive the highest level of recommendation (class I) for CRT.
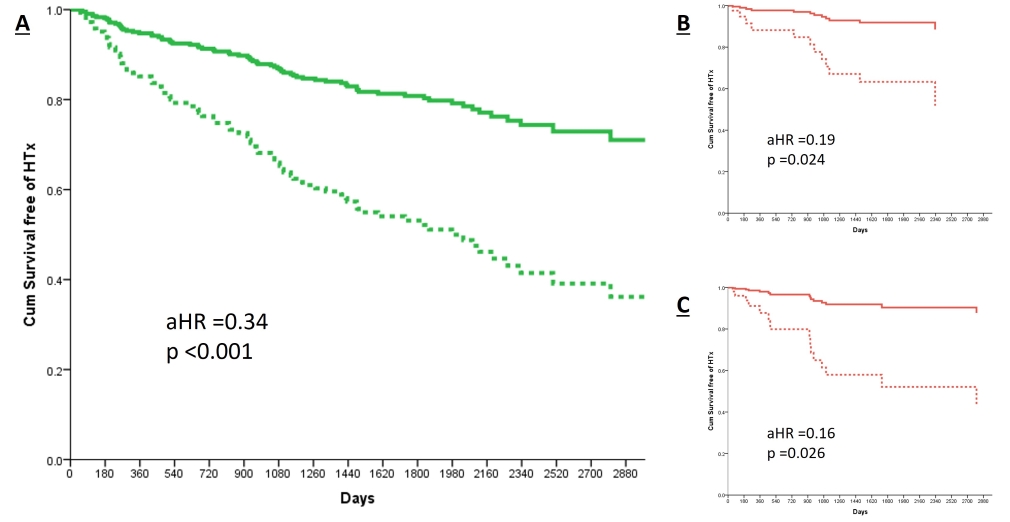
Figure 1 - Adjusted cumulative survival curves for overall survival free of heart transplant stratified by SFoAR. The solid-coloured lines represent the patients with SFoAR. The dotted coloured line represents the patients without SFoAR. The hazard ratios and p-value were obtained using multivariate cox regression analysis. The models were adjusted for QRS duration and QRS morphology in addition to age, gender, atrial fibrillation/flutter, ischemic heart disease, and use of a defibrillator.
A) Full cohort B) patients with QRS duration 130-149ms C) patients with non-LBBB morphology
Figure 1 - Adjusted cumulative survival curves for overall survival free of heart transplant stratified by SFoAR. The solid-coloured lines represent the patients with SFoAR. The dotted coloured line represents the patients without SFoAR. The hazard ratios and p-value were obtained using multivariate cox regression analysis. The models were adjusted for QRS duration and QRS morphology in addition to age, gender, atrial fibrillation/flutter, ischemic heart disease, and use of a defibrillator.
A) Full cohort B) patients with QRS duration 130-149ms C) patients with non-LBBB morphology
aHR = adjusted hazard ratio; HTx = heart transplant; non-LBBB = non left bundle branch block; SFoAR = septal flash or apical rocking