1Herzzentrum Leipzig - Universität Leipzig Klinik für Innere Medizin/Kardiologie Leipzig, Deutschland; 2Universitätsmedizin der Johannes Gutenberg-Universität Mainz Mainz, Deutschland; 3Universitätsmedizin der Johannes Gutenberg-Universität Mainz Kardiologie 1, Zentrum für Kardiologie Mainz, Deutschland
Background: Diastolic function has recently been acknowledged as a key pathognomonic factor in patients with severe tricuspid regurgitation (TR) undergoing transcatheter edge-to-edge repair (T-TEER). We therefore aimed to investigate the role of left atrial reservoir strain (LARS), as surrogate for diastolic function, in patients undergoing T-TEER.
Methods: Patients undergoing T-TEER between 2016 to 2019 in our institution were included in the present study. LARS was derived from 2-D-speckle-tracking. Patients were grouped according to LARS median. The primary outcome was one-year all-cause mortality.
Results: Overall, 100 patients were available for analysis, whereas 5 patients that presented with sinus rhythm were excluded from the analysis. The remaining 95 patients represented typical characteristics of patients undergoing T-TEER with high age (median 79, IQR 76 to 86 years), increased perioperative risk (EuroSCORE II 4.7, IQR 2.9 to 8.6%) and high symptomatic burden (63% NYHA class ≥III). T-TEER was successful in all cases and 86% had a residual TR ≤ II (on a V grade scaling scheme).
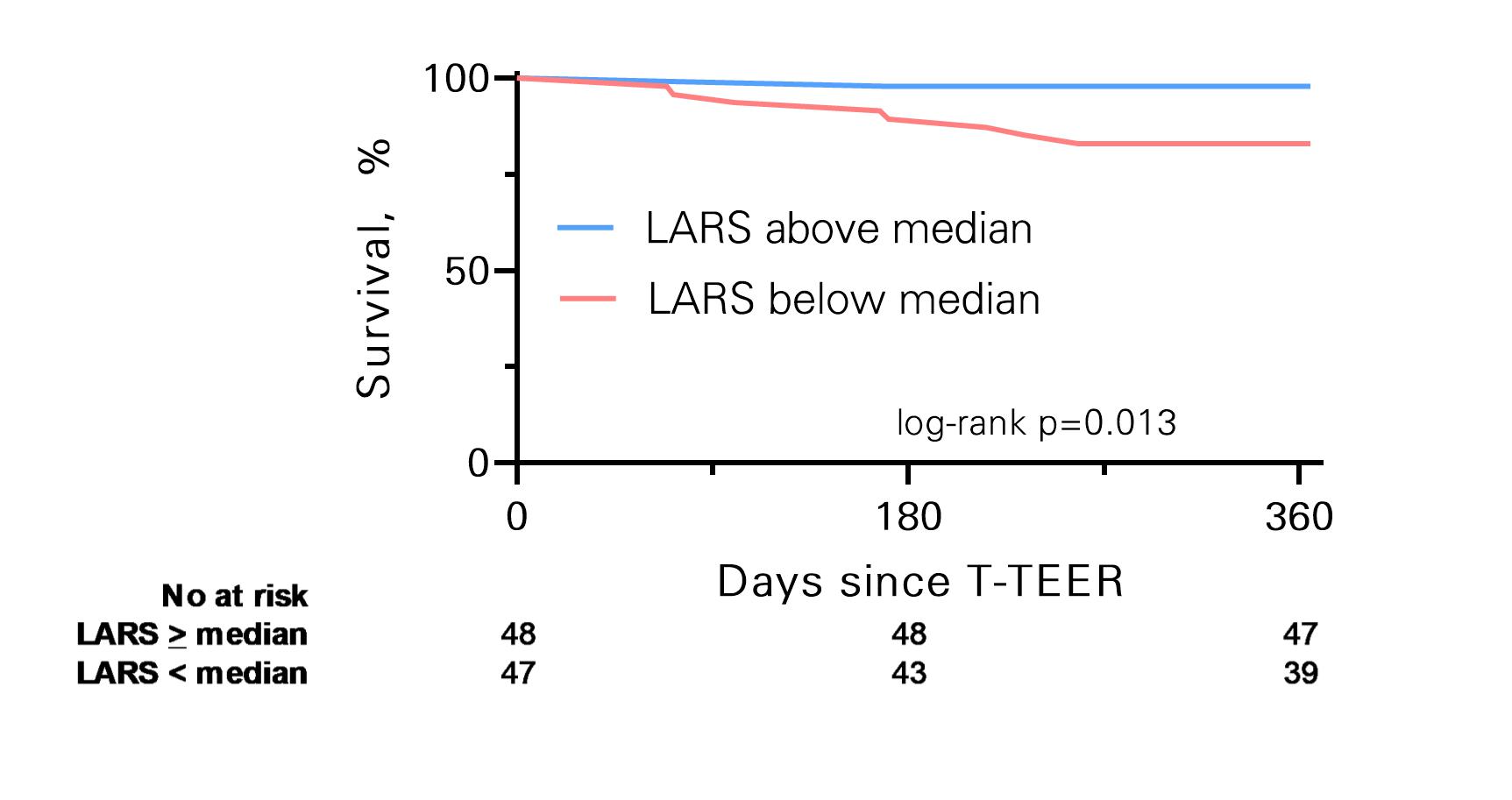
T-TEER patients presented with severely dilated LA (left atrial volume index [LAVI] 49, IQR 34 to 67 ml/m²), reduced LA ejection fraction (32, IQR 18 to 43%) and relevantly impaired LARS (8.4, IQR 5.8 to 12.0%). Within the one-year follow-up 9 (10%) of patients died. All-cause mortality occurred significantly higher in patients with a LARS below the median of 8.4% (Figure 1, p-log rank = 0.013). Interestingly neither LAVI (hazard ratio 0.99, 95% CI 0.96 to 1.02) nor the LA ejection fraction (HR 1.00, 95% 0.97 to 1.05) were associated with the primary outcome, while LARS remained associated, even after adjustment for residual TR (HRadj 8.7, 95% CI 1.09 to 70).
Conclusion: LARS is severely impaired in patients undergoing T-TEER and is associated with one-year morality independently of residual TR.